Kieferorthopädie und mandibuläre orthognathische Chirurgie
Maschinenübersetzung
Der Originalartikel ist in ES Sprache (Link zum Lesen) geschrieben.
Klinischer Fall
Die 20-jährige Patientin kam besorgt über die Beweglichkeit eines Milchzahns, den Überbiss und die Abweichung der unteren Mittellinie nach einer vorherigen kieferorthopädischen Behandlung in das Kieferorthopädiezentrum.
Es wurde eine umfassende Diagnose des knöchernen und zahnärztlichen Problems in den drei Raumebenen sowie der parodontalen und gelenklichen Gesundheit durchgeführt, nach der die verschiedenen Behandlungspläne mit ihren jeweiligen Vor- und Nachteilen erläutert wurden. Da die Zusammenarbeit mit dem Kiefer-Gesichtschirurgen bei einem der Pläne unerlässlich war, wurde die Patientin zur Kiefer-Gesichtschirurgie überwiesen, wo sie über die potenziellen Vorteile und Nebenwirkungen der kombinierten Behandlung informiert wurde.
Anamnese:
- Name: E.C.
- Alter: 20 Jahre und 8 Monate.
- Medizinische Vorgeschichte: Ohne Interesse.
- Grund der Konsultation: Beweglichkeit eines Milchzahns, Überbiss und Abweichung der unteren Mittellinie.
Diagnose
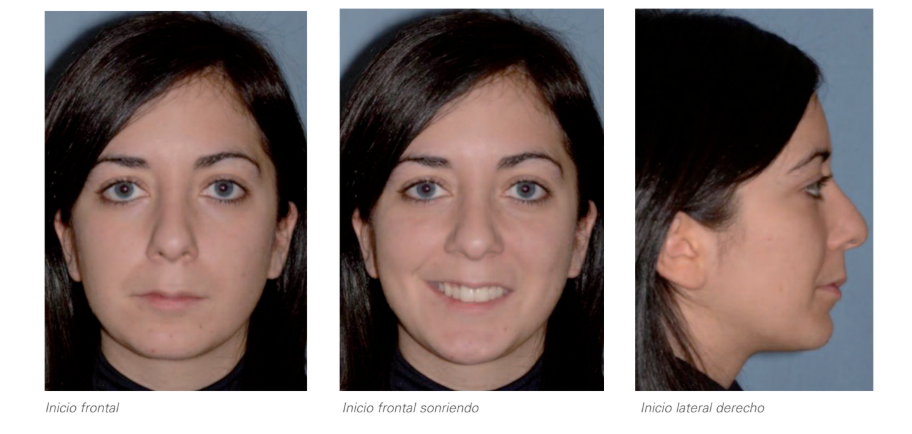
1. Extraorale Analyse:
Unteres Drittel leicht kleiner als das mittlere Drittel.
Angemessene Exposition der Schneidezähne in Ruhe und beim Lächeln.
Asymmetrisches Lächeln aufgrund unzureichender Hebung des linken Mundwinkels.
Konvexes Profil.
Unterer Rückbiss.
Kinn leicht retrognath.
Ausgeprägter mentolabialer Winkel.
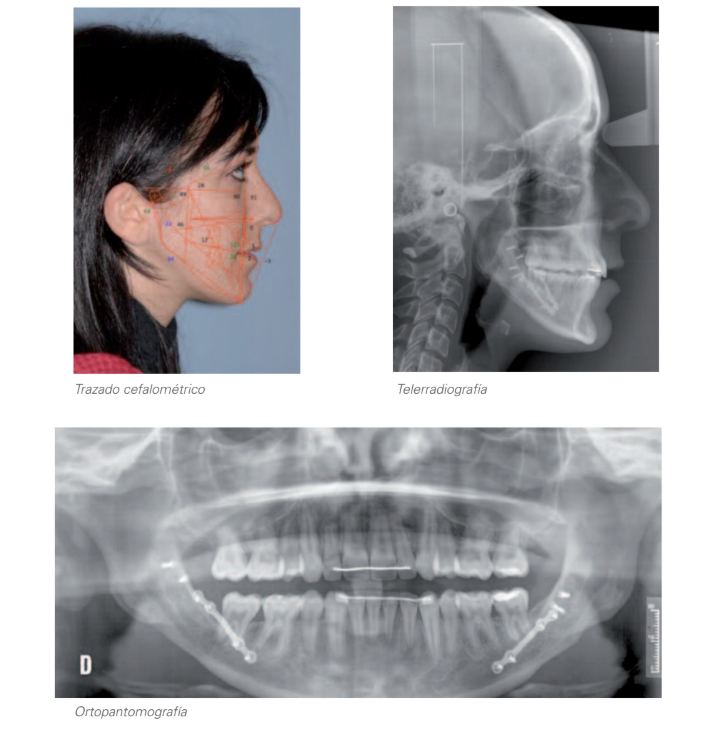
2. Röntgenanalyse:
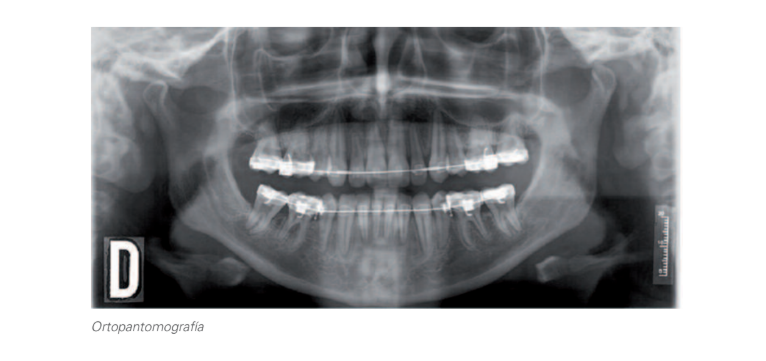
2.1. Orthopantomographie:
- Permanente Dentition.
- Rechter Kondylus kleiner als der linke.
- Agenesie des 45.
- Fehlen von: 18, 14, 24, 28, 35 und 48.
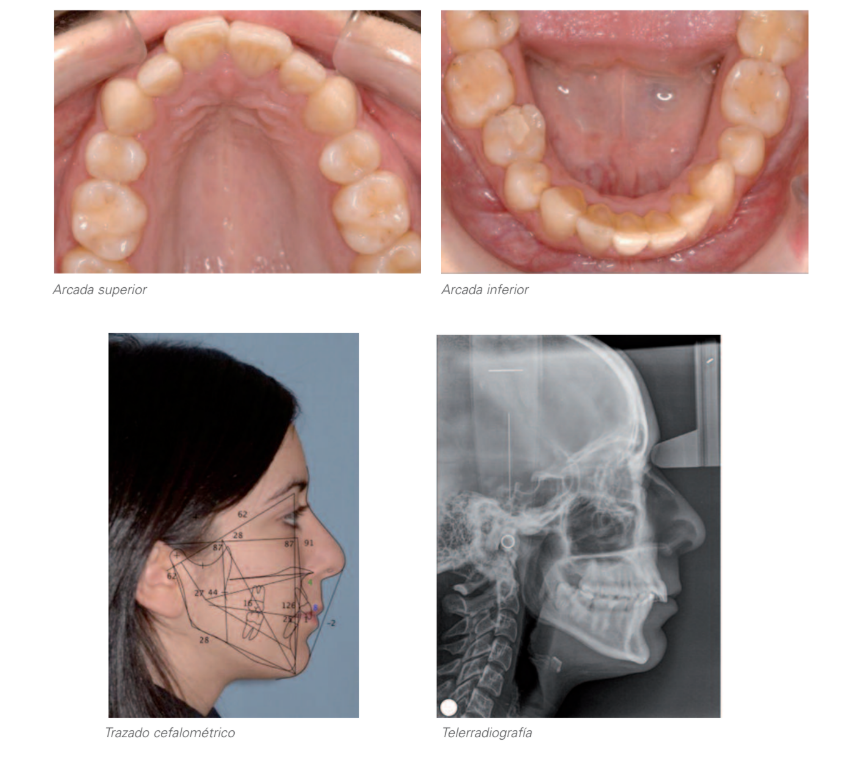
2.2. Laterale Tele-Röntgenaufnahme des Schädels und cephalometrische Zeichnung:
- Mesofazial.
- Klasse II knöchern aufgrund mandibulärer Ursachen.
- Schneidezähne korrekt in Bezug auf ihre knöchernen Basen positioniert.
3. Intraorale Analyse:
- Abweichung der unteren Mittellinie nach links um 1,5 mm aufgrund zahnärztlicher Ursachen (asymmetrische Unterkieferbögen als Folge einer vorherigen kieferorthopädischen Behandlung, die asymmetrische Zahnextraktionen im Unterkiefer beinhaltete, wobei der 85 trotz Agenesie erhalten blieb).
- Kreuzbiss von 46-16 und 17 aufgrund zahnärztlicher Ursachen (übermäßige koronovestibuläre Torsion des 46 und Lage außerhalb der Bogenlinie).
- Überbiss: 5 mm.
- Rechte Seite: Klasse II vollständiger Molar und Klasse I Canine.
- Linke Seite: Klasse II Molar und vollständige Klasse II Canine.
- Überbiss: 4,5 mm.
- Vorhandensein von Zahnstein auf der Lingualseite des anterioren Unterkiefers.
Erstuntersuchung


Behandlungsplan
Der erste Schritt vor Beginn der Behandlungsplanung besteht darin, die Behandlungsziele für jeden einzelnen Fall zu bestimmen, die sich auf die jeweiligen Bereiche konzentrieren, die potenziell von der vorgeschlagenen Behandlung betroffen sind. Diese Ziele bilden gleichzeitig einen Referenzrahmen sowohl für den Patienten als auch für die verschiedenen Fachleute und sind ein kritisches Element zur Bewertung der Ergebnisse, die am Ende der Behandlung erzielt werden. Diese Ziele sind:
- Gesichtsästhetik.
- Zahnästhetik.
- Funktionelle Okklusion.
- Parodontalgesundheit.
- Stabilität.
Zufriedenheit mit dem Grund des Patientenbesuchs. Basierend darauf wurden 2 Behandlungsoptionen bewertet:
Option A: Behandlung nur mit Kieferorthopädie
- Tartratzentfernung.
- Wiedereröffnung des Raums zwischen dem linken unteren Eckzahn und dem linken unteren ersten Prämolaren, mit dem Ziel, den Überbiss, die linke canine Klasse II zu korrigieren, Symmetrie im Unterkiefer zu erreichen und die mittleren Zahnlinien zu zentrieren.
- Extraktion des rechten unteren temporären zweiten Molaren und Schließung des Raums bis zur Erreichung einer identischen Größe wie auf der gegenüberliegenden Seite.
- Korrektur des rechten hinteren Kreuzbisses, Verbesserung des Torques des 46 und Rückführung an seinen Platz im Zahnbogen.
- Im letzten Fall wäre es notwendig, die Räume im dritten und vierten Quadranten zu rehabilitieren.
- In Bezug auf die möglichen Auswirkungen auf die zuvor genannten Behandlungsziele wurde das Potenzial schädlicher Effekte auf die parodontalen Gesundheit aufgrund der Notwendigkeit, die unteren Schneidezähne übermäßig zu protrudieren, sowie die Möglichkeit, sie zu stark in Bezug auf die vestibuläre Kortikalis zu drücken, sowie in Bezug auf die Gesichtsästhetik, da der mentolabiale Winkel betont wird, bewertet. Außerdem wurde das niedrige Maß an Vorhersehbarkeit hinsichtlich der Erreichung der Ziele auf okklusaler Ebene sowie ein erhöhtes Risiko für Rückfälle aufgrund der unvermeidlichen übermäßigen Vestibulierung des antero-inferioren Sektors berücksichtigt.
Option B: Kombinierte Behandlung mit Kieferorthopädie und Kieferchirurgie
- Tartratzentfernung.
- Entfernung des zweiten unteren rechten Milchmolars, um Symmetrie im Unterkiefer zu erreichen, die mittlere Zahnlinie des Unterkiefers mit der des Oberkiefers zu zentrieren und die skeletale Klasse II zu kompensieren.
- Korrektur des rechten hinteren Kreuzbisses, Verbesserung des Torques des 46 und Rückführung an seinen Platz im Zahnbogen.
- Entfernung des 38.
- Anschließend würde eine Kieferchirurgie zur Vorverlagerung des Unterkiefers durchgeführt, um die Gesichtsästhetik der Patientin zu harmonisieren und einen angemessenen Grad an Überbiss und Überbiss zu erreichen, sowie eine vollständige bilaterale Klasse I für die Eckzähne und Klasse II für die Molaren.
- Schließlich würde die Phase der Settling und Fertigstellung beginnen, um alle Behandlungsziele auf okklusaler Ebene zu erreichen.
- Mit dieser Option würden alle Behandlungsziele erreicht.
Die Patientin entschied sich für die Option B, hauptsächlich motiviert durch den höheren Grad an Compliance in Bezug auf die festgelegten Behandlungsziele.
Präoperative Studie


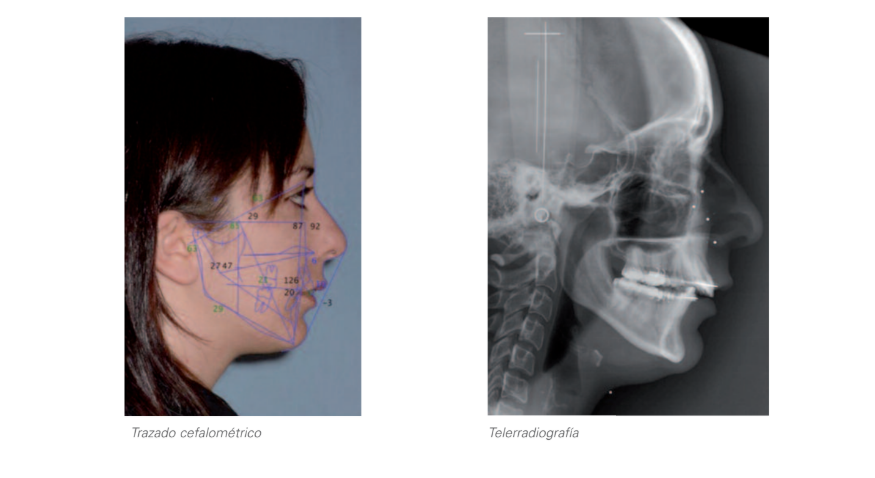
Chirurgie
Unter Allgemeinanästhesie wurde eine nasotracheale Intubation durchgeführt. Es wurde eine sagittale Mandib osteotomie nach Obwegesser-Dalpont-Epker durchgeführt, die zur Erzielung einer guten Kontaktfläche bis distal des 2. Prämolars geführt wurde.
Der distale Fragment wurde umfangreich freigelegt, um einen spannungsfreien Vorschub zu erreichen. Eine Schiene wurde an der Stelle platziert, an der die Osteotomie fixiert werden sollte.
Die Frakturen wurden mit 2 mm Miniplatten und Klasse II bikortikalen Schrauben fixiert, nachdem die passive Anpassung der Schiene überprüft wurde.
Die Patientin wurde im Operationssaal extubiert und 24 Stunden später entlassen.
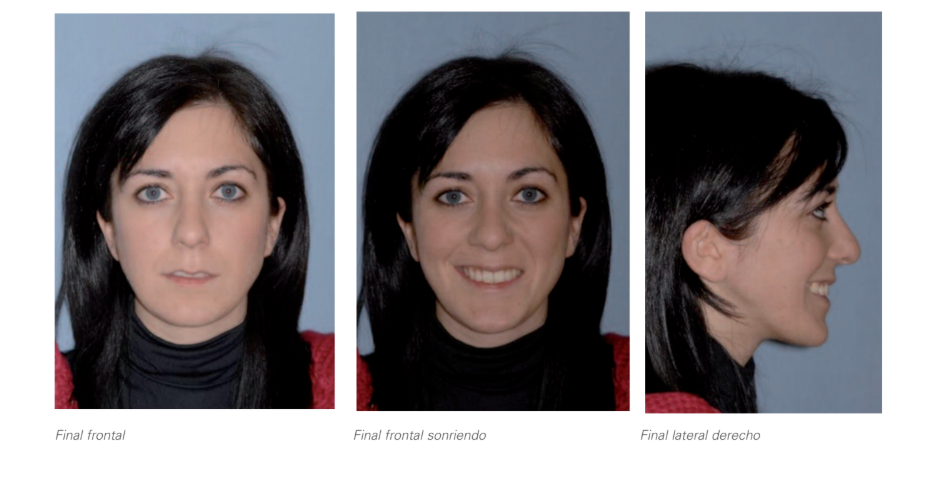
Abschlussstudie



Diskussion
Die Klasse II ist die häufigste Malokklusion in der Kieferorthopädie und wird auch in einem höheren Prozentsatz der Fälle von Kieferchirurgen behandelt. Es wird geschätzt, dass etwa 5% der Kaukasier anfällig für einen mandibulären Vorstoß sind. Gewöhnlich ist die Klasse II kein reines sagittales Problem, sondern ist mit einem vertikalen Problem assoziiert, wobei der häufigste Fall ein übermäßiger vertikaler Oberkiefer mit oder ohne offene Biss ist. Der mandibuläre Vorstoß erfolgt durch die sagittale Osteotomie des Astes. In Fällen der monomaxillären mandibulären Chirurgie bestimmt die Größe des Überbisses das Ausmaß des Vorstoßes der Mandibel, und es ist daher entscheidend, dass der Kieferorthopäde den notwendigen Überbiss schafft, indem er gleichzeitig die dentoalveolären Kompensationen beseitigt. In den Fällen, in denen es erforderlich ist, wird eine Mentoplastik eingesetzt, um das angemessene ästhetische Ergebnis zu erzielen. Mandibuläre Vorstöße sind vorhersehbar mit einem kleinen Rückfallprozentsatz, wenn sie erfolgreich durchgeführt werden.
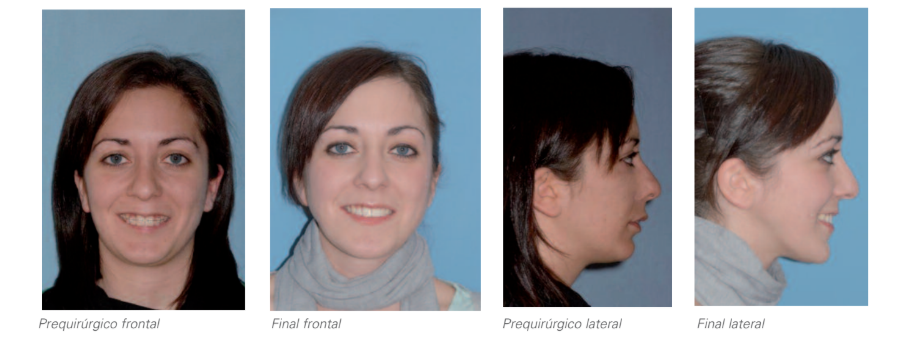
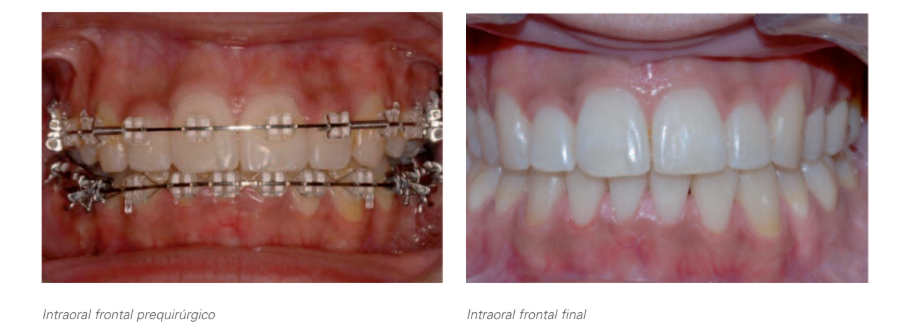
Vergleich präoperativ/endgültige Situation
Javier Prieto Serrano, César Colmenero Ruiz, Fe Serrano Madrigal, Teresa Martínez Iturriaga
Bibliografie
- Epker BN. Modifikationen in der sagittalen Osteotomie des Unterkiefers J. Oral Surg. 1977 35-157-159.
- Obwegsseer H. Eingriffe am Oberkiefer zur Korrektur der Prognathie. Zahnheilk 1965; 75: 356.