
en
Root canal passage
27
7 Min Lesezeit
18 Mai 2018
Maschinenübersetzung
Der Originalartikel ist in RU Sprache (Link zum Lesen) geschrieben.
Pre-bending of the tool creates conditions for safer use of hand files and rotary NiTi tools. Root canal scouting is the first stage of instrumentation, during which procedural difficulties or errors can most often arise.
About the passage of canals of complex configuration at the webinar Extreme in endodontics or C-shaped canals .
Forms of root canals and their treatment
The coronal 2/3 passage provides information about the anatomy of the root canal system and provides important information about the degree of canal curvature, whether canals are backward curving, or whether there are gaps. Clinicians should evaluate five common root canal anatomical shapes. These can be channels that join together, bend, bend back, or separate.
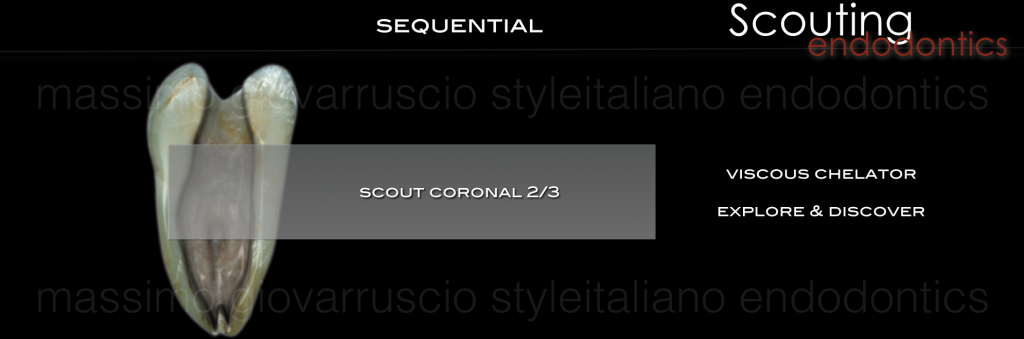
Photo 1.
When the direct approach (straightline) is completed and all holes are found, all attention is directed to preparing the root canal. If the pulp is alive and bleeding, then the chamber is filled to the brim with a viscous chelate. If the pulp is necrotic, then the chamber is irrigated and completely filled with a 5.25% warm NaOCL solution. As they pass, smaller stainless steel files are measured on a diagnostic x-ray and pre-bent to exactly match the expected length and curvature of the root canal. Tapered stainless steel hand K-files with a diameter of 0.02 are used to penetrate the coronal 2/3 of the root canal.
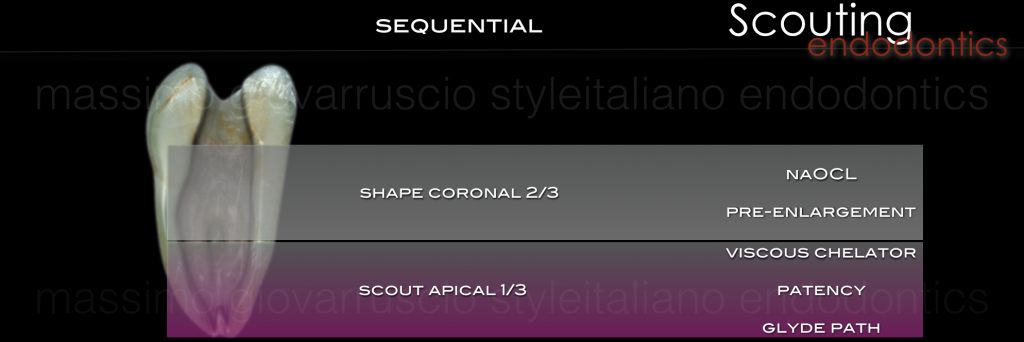
Figure 2. After completion of the coronal 2/3, the canal is irrigated with NaOCL and can be pre-expanded using hand instruments, gates-gliden or rotary NiTi processing files. When the coronal 2/3 are well treated mechanically and medicinally, then we proceed to the treatment of the apical 1/3. Small hand files (K-files number 8 or 10) are used to traverse the rest of the canal, creating a carpet.

Photo 3. In canals with complex anatomy with small, long and potentially branched canals, it is not possible to immediately pass a 10 K file to the end of the root. Subsequently, the clinician may attempt to use smaller files at the apex when traversing the canals. Usually K-files 06 and 08 are not needed to widen the canal in the apex area, unless, of course, this is a very difficult case.

Photo 4: The apical foramen will always be larger than the size of a 10 K file, so any resistance encountered at the apex will likely be due to a bowed or abnormally shaped canal. Opening the canal with a 10 K file with a slight build-up can be an effective way to stay on track while minimizing the chance of creating a ledge or blocking the canal.

Photo 5: A passing tip is that the file should never be forced apically as the risk of creating ledges is greatly increased. If the tip of the file never touches the canal walls, it is impossible to create a projection.

Figure 6: Postoperative radiograph shows how the original anatomy was preserved after root canal instrumentation. Precurving and traversing the canal ensures that the entire anatomy of the root canal is preserved.
Passing channels with obstacles
Canals can also be combined with various anatomical obstructions, such as a straight canal with an irregular apex, a curved canal with an irregular shape, and a sharply curved canal.

Photo 7.
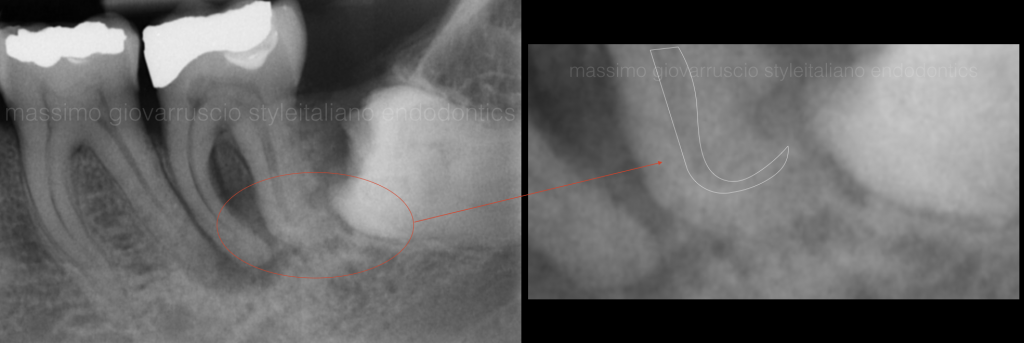
Photo 8. These channels require skill and persistence to navigate. Obstacles are identified tactilely (felt through the handle of the file) by the presence of “weak resistance” at the top of the file. This happens because the tip of the file gets stuck, rather than grinding along the length and further.
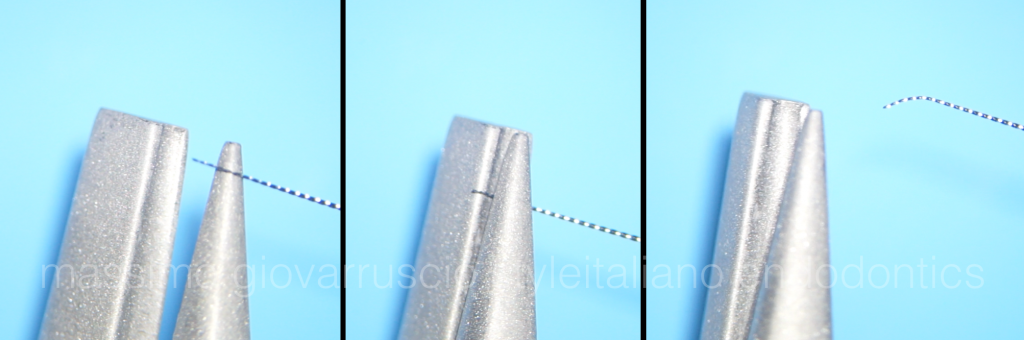
Photo 9: When an apical obstruction is identified, remove the file, smoothly bend the last 2mm using a file bending tweezers (EndoBender), align the silicone stopper mark with the file bend and you will be able to overcome the obstruction.
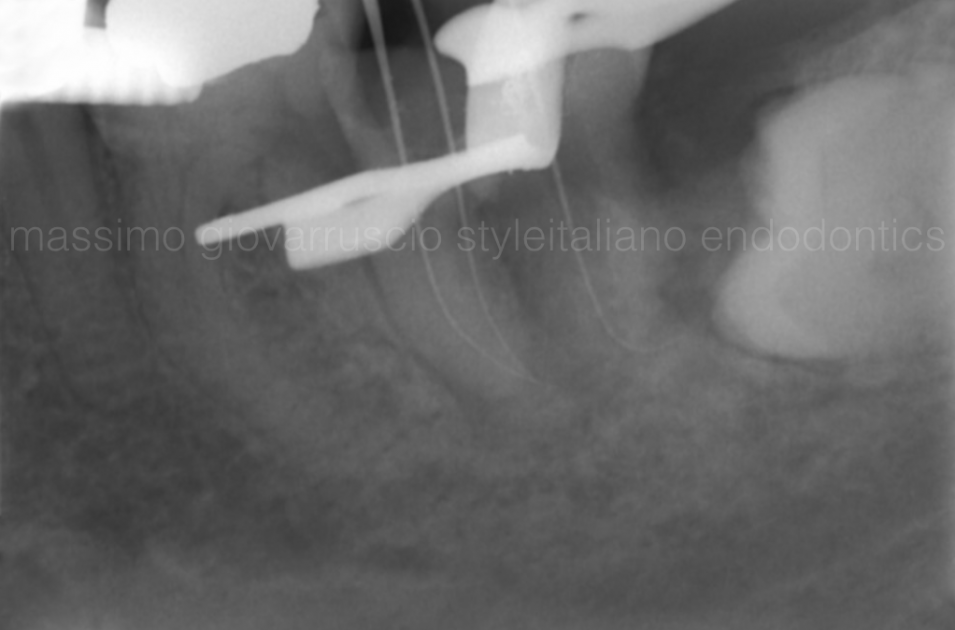
Photo 10: When passing through the canal, be careful with the rotational movements used to move the file through the obstruction. When you encounter an obstacle, you should remove the tip of the file 1 mm and turn it in a new direction. Move it apically with a rocking motion and see if it moves. If not, pull back, redirect the tip of the curved file and see if it falls out. Repeat until apical advancement is observed and access is achieved. An apex locator and radiograph are needed to verify whether the end point has been reached after successfully passing the obstacle.

Figure 11: Postoperative radiographs show complete three-dimensional filling of the root canal and adherence to complex anatomy.

Photo 12. In difficult cases, many attempts may be required when passing through the channels. Once the tip of the file goes beyond the obstruction, it will sink deeper into the canal.
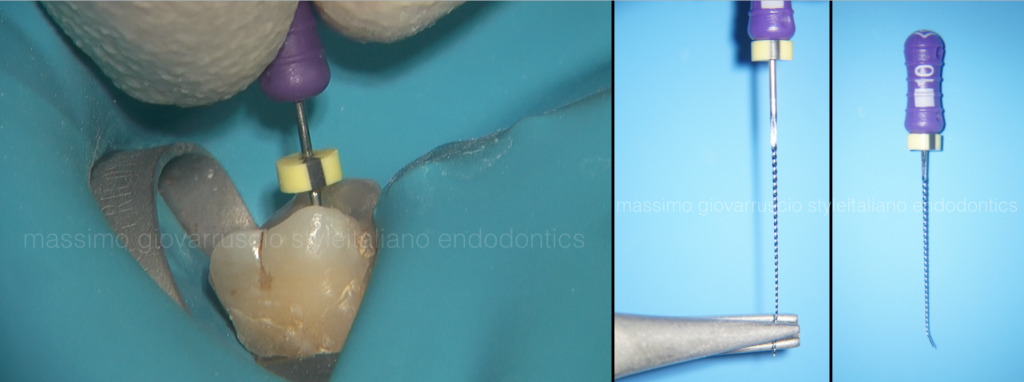
Photo 13: During passage, a mark on the silicone stopper informs the clinician of the direction of the curved file tip as it crosses the obstruction, indicating its path. As you bend the file and move deeper, use the apex locator as you work through it until the required distance is achieved.
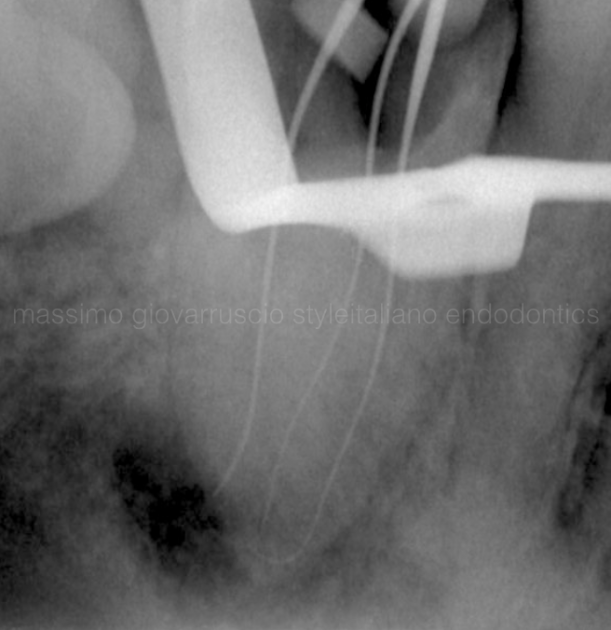
Photo 14. Once past the obstruction, do not remove the file from the canal, as it will inevitably straighten and will no longer move through it without being completely removed, bent, and reinstalled.
In a channel with a double obstruction, such as an S-shaped channel, its volume will decrease in the direction of the first bend. The file will then again experience a decrease in resistance relative to the apex when it encounters the second bend of the canal. In this case, pull the file back slightly, rotate it 180 degrees, wiggle it and see if it catches or just drops along its length.

Photo 15: With the curved files and indicators on the stoppers, you should be able to mentally map the path of the channel around the obstacles, then easily move around them and get the job done!
Channel passage
This article describes the rationale for passing and then pre-expanding the coronal 2/3 of the canal before completing the passage of the apical 1/3. The passage of the canal has a decisive influence on the creation of an acceptable and safe carpet.
Learn more about the features of processing canals with complex anatomy in the online course Endodontics today: expert protocols and new perspectives .
http://www.styleitaliano.org/
Melden Sie sich an oder erstellen Sie ein Konto, um den gesamten Artikel zu lesen. Es ist kostenlos
Um weiterzulernen und Zugang zu allen anderen Artikeln zu erhalten, melden Sie sich an oder erstellen Sie ein Konto
