Chirurgie der Klasse-III-Malokklusion: Wann nur eine Kieferoperation durchführen?
Maschinenübersetzung
Der Originalartikel ist in ES Sprache (Link zum Lesen) geschrieben.
Anamnese
Der 26-jährige Patient kam zur Konsultation wegen chirurgischer Behandlung seiner Kieferdeformität. Der Patient klagte über einen großen Kiefer und Beschwerden im linken Kiefergelenk.
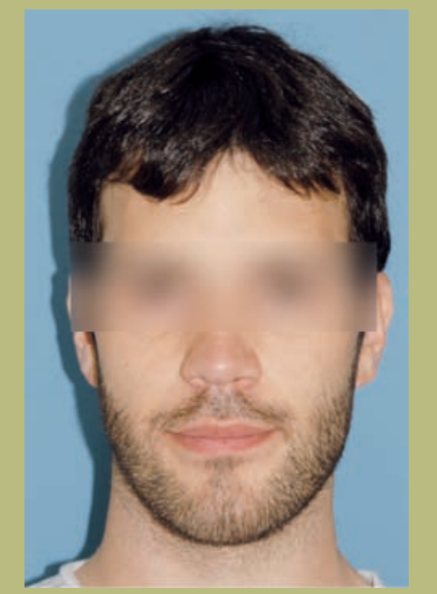
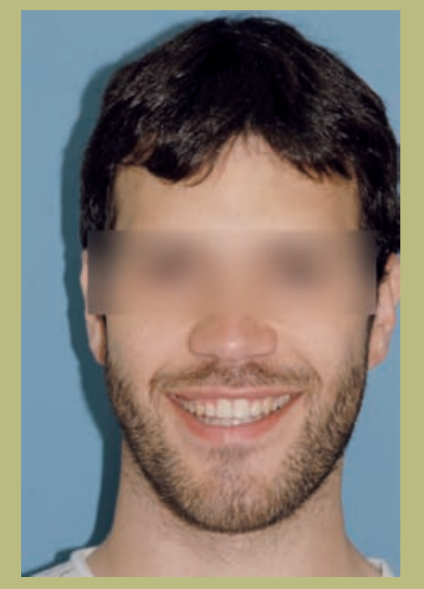
Gesichtsanalyse
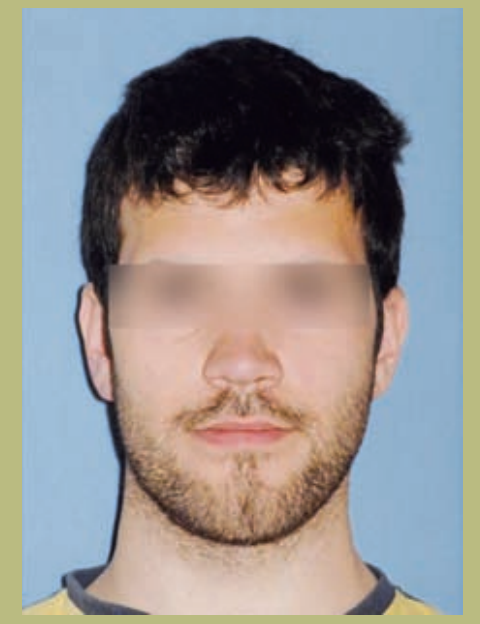
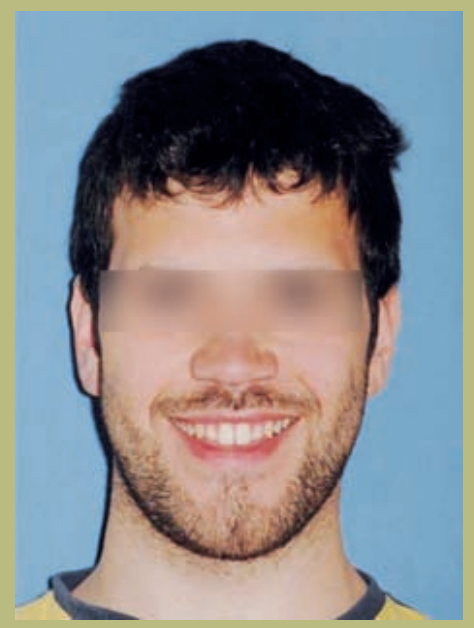
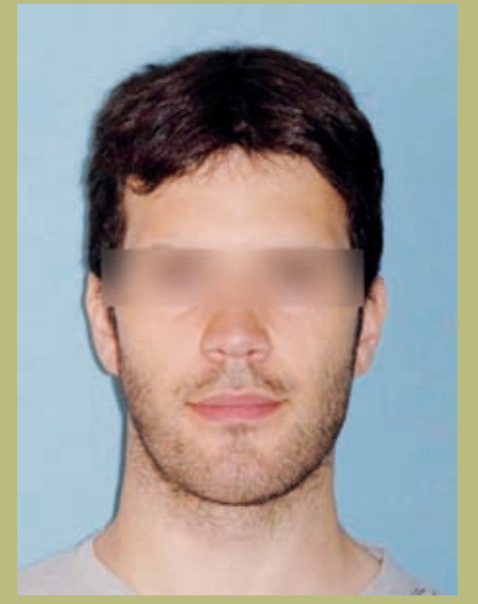
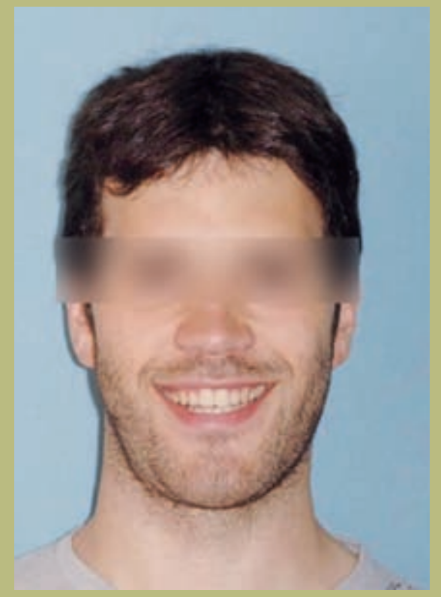
- Stirn (Abbildungen 1 und 2)
- Leichte Exposition der Sklera.
- Normale bimaxilläre Breite.
- Flache paranasale Konfiguration (Hypoplasie der paranasalen Bereiche).
- Die Nasenlöcher und der interalar Abstand sind verbreitert.
- Leichte Kieferasymmetrie.
- Langes Gesicht mit einem Gefühl von vertikaler Zunahme des Kinns.
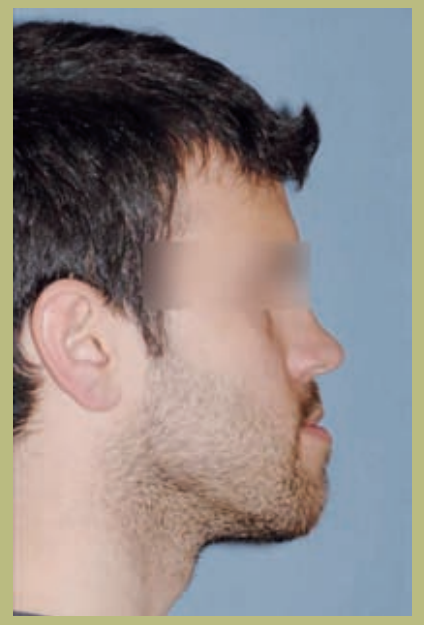
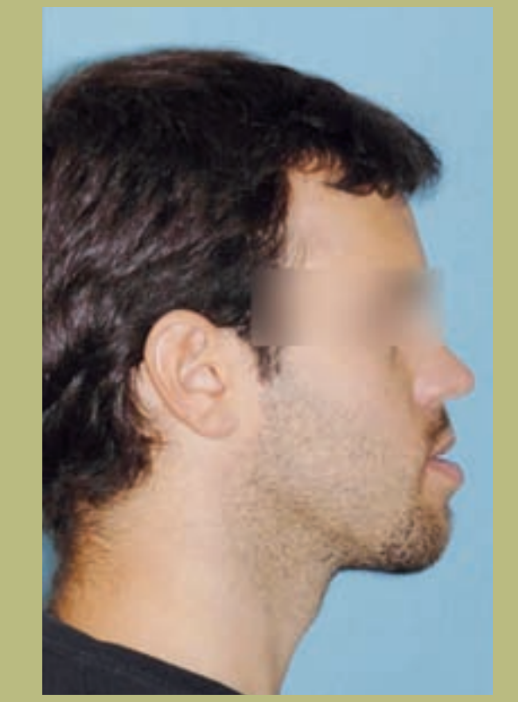
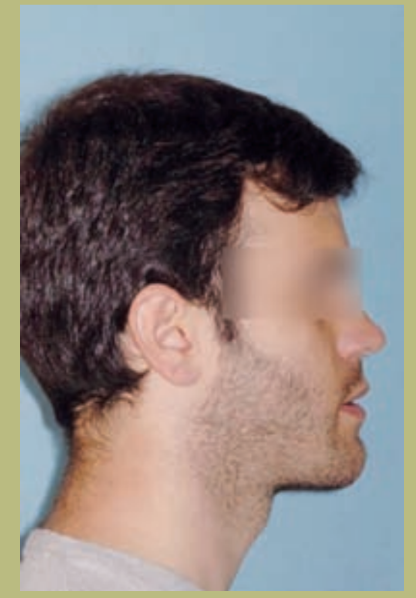
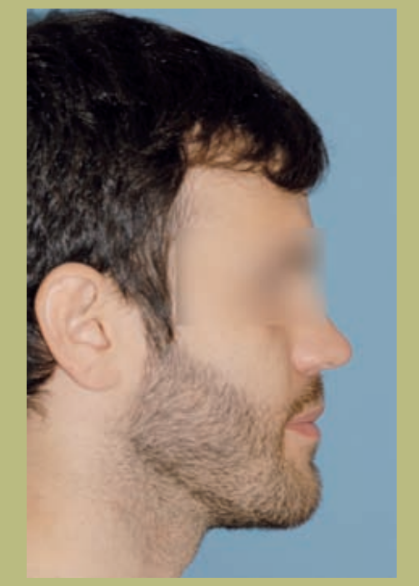
Profil (Abbildung 3)
- Verminderte Projektion des infraorbitalen Randes.
- Flache Wangenkonfiguration.
- Flache paranasale Konfiguration.
- Normale Nasengröße mit leicht erhöhtem nasolabialem Winkel.
- Erhöhte cerviko-mentale Länge.
- Normaler cerviko-mentaler Winkel.
- Verminderte mentolabiale Furche.
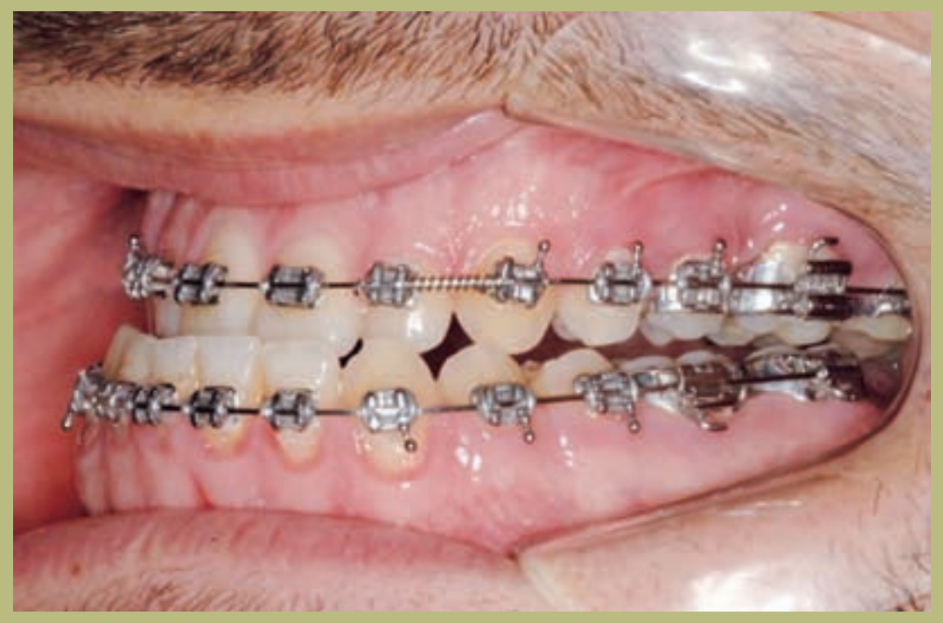
Intraorale Analyse (Abbildungen 4–8)
- Klasse III molar und canine vollständig rechts und links.
- Vorderer Kreuzbiss mit einem Überbiss von -7 mm.
- Überbiss 2 mm.
- Drehung 16, 26, 25.
- Abweichung der unteren Mittellinie nach rechts von 1,5 mm.





Radiologische Analyse (Abbildungen 9–11)
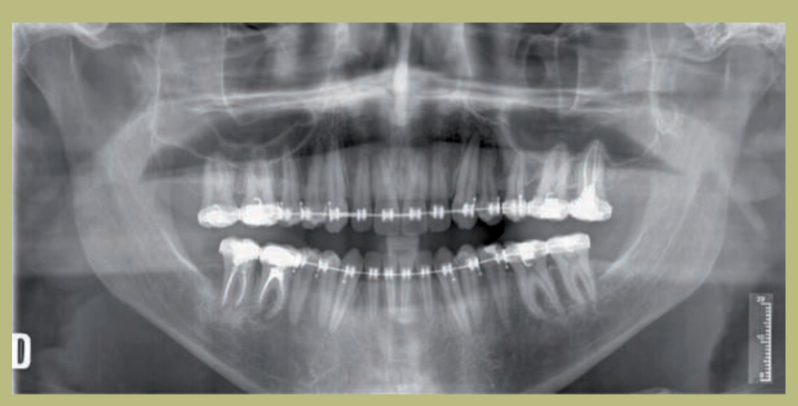
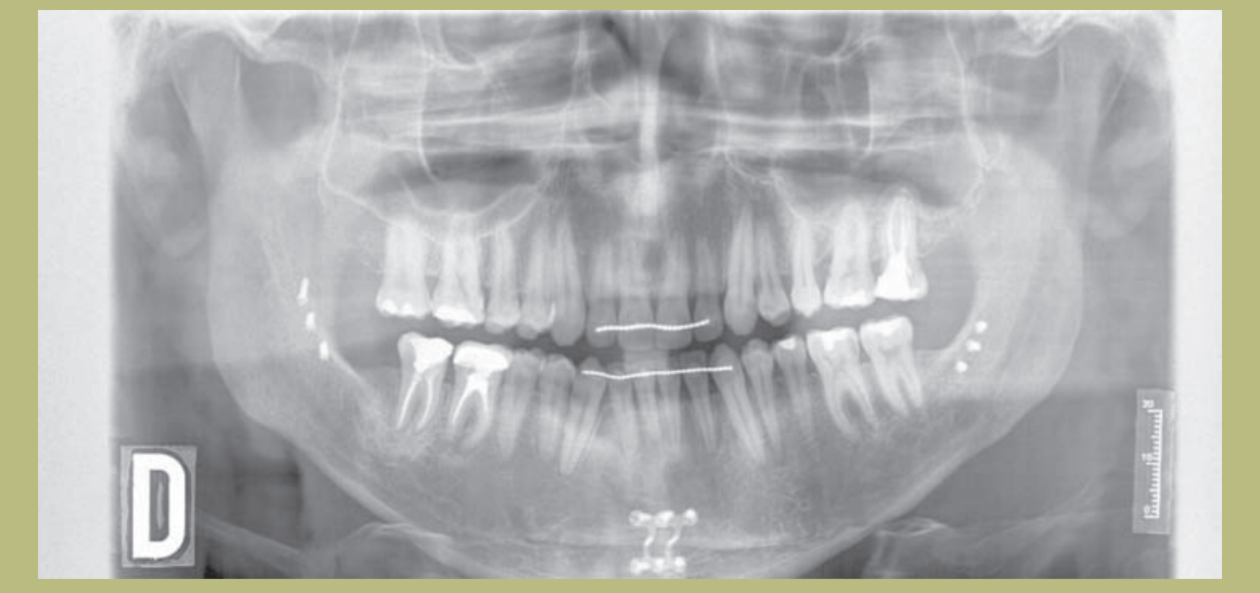
1) Orthopantomographie:
- Winkeliger Knochendefekt des 26.
- Extrusion des 17.
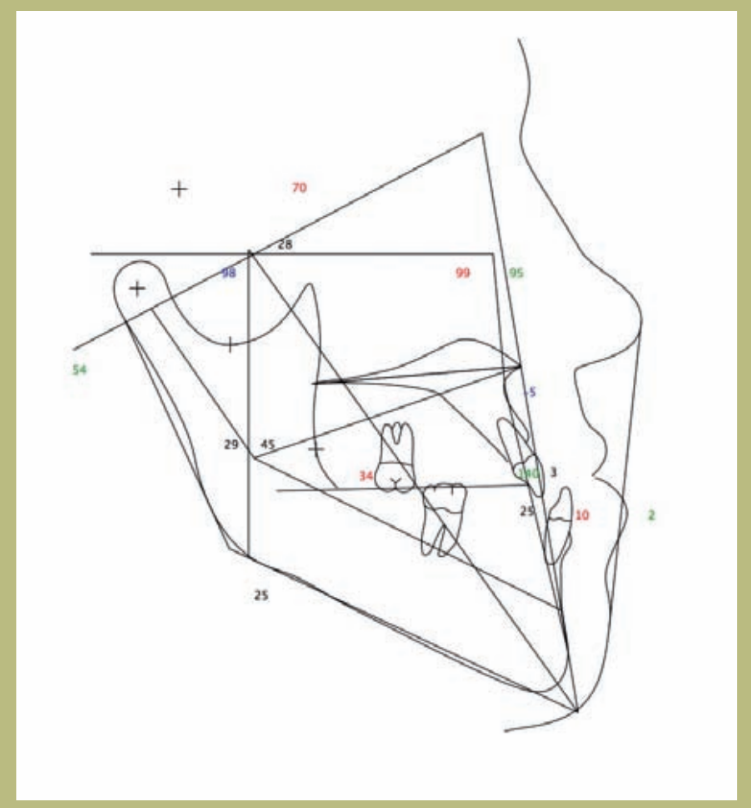
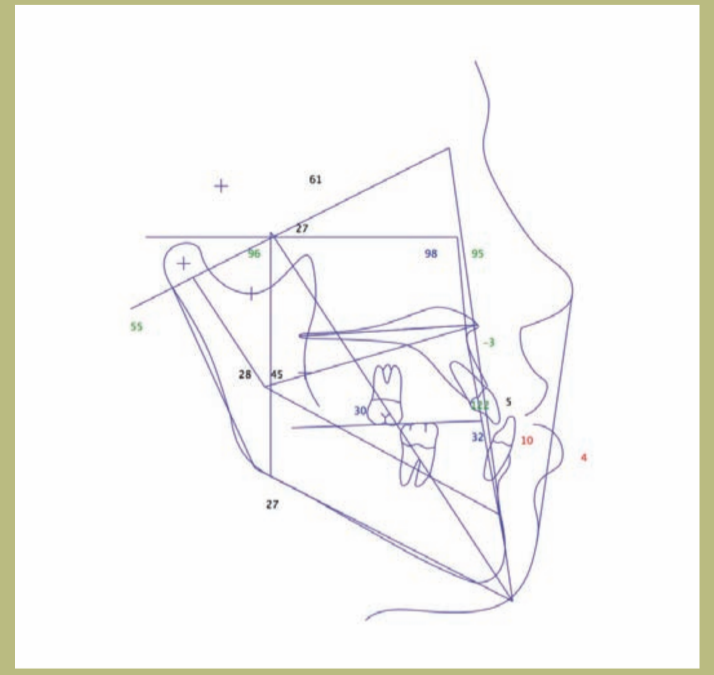
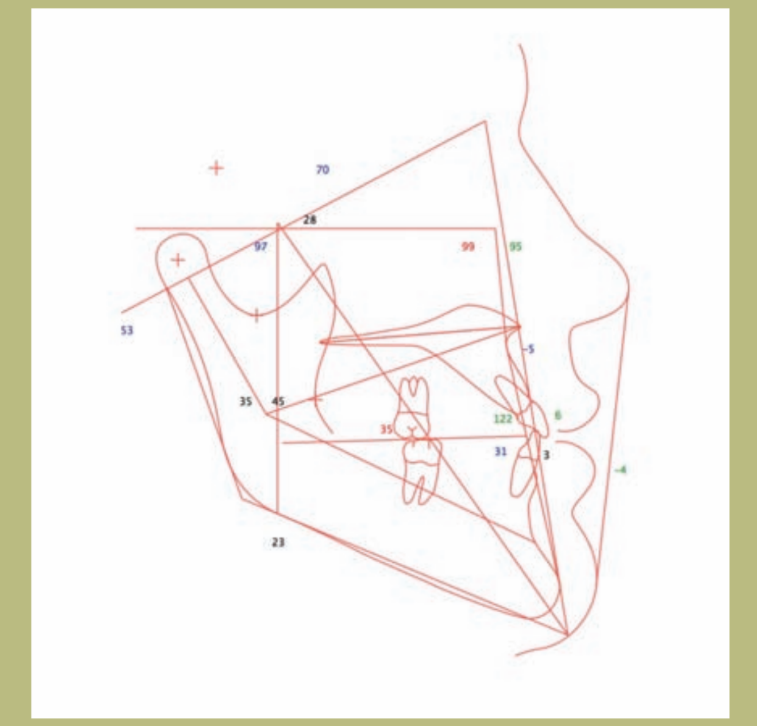
2) Cephalometrie:
- Skelettale Klasse III mit gemischter Herkunft (maxilläre Hypoplasie und mandibuläre Hyperplasie).
- Obere Schneidezähne korrekt auf ihren knöchernen Basen positioniert und die unteren leicht lingualisiert.


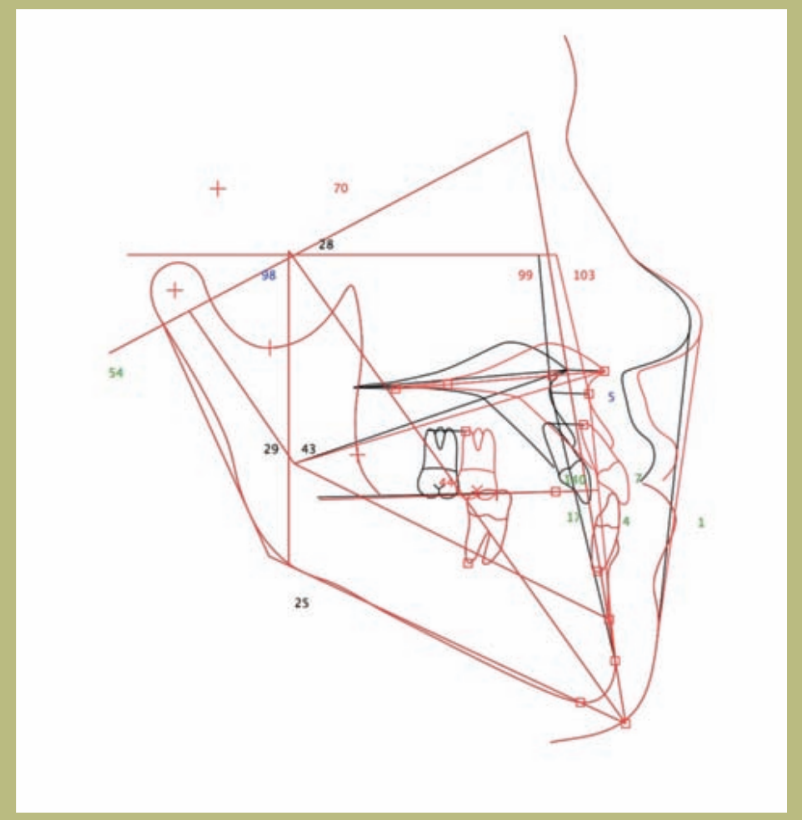
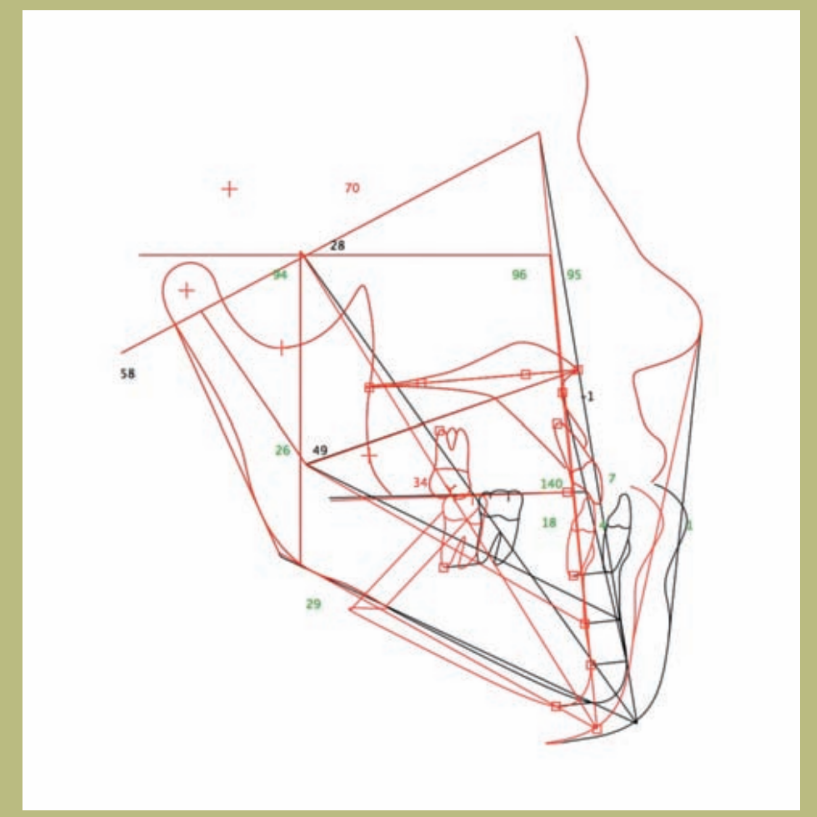
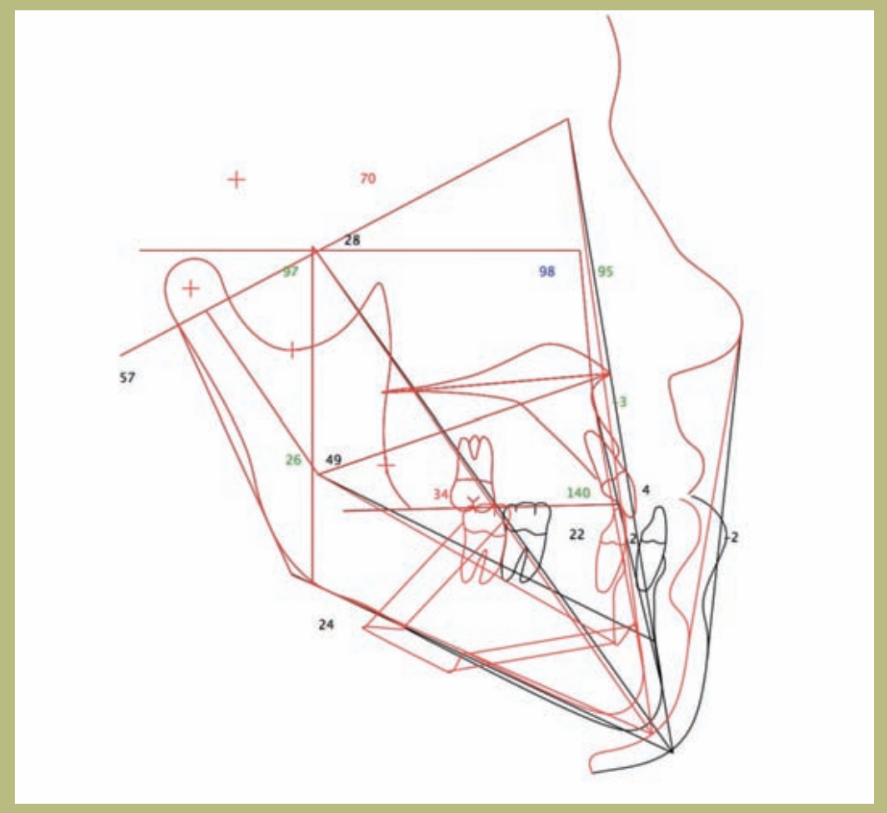
V.T.O. (Abbildungen 12–14)
1) Wenn ausschließlich ein maxillärer Vorstoß durchgeführt wird, treten mehrere potenzielle Probleme auf. Einerseits ist der Vorstoß sehr groß (10 mm) und andererseits würde dies einen sehr ungünstigen Effekt auf die Nase und ihr Fundament haben, was zu einem sehr offenen nasolabialen Winkel (über 105 Grad) und einer schwer chirurgisch zu behandelnden Erweiterung der alar Basis führen würde; außerdem würde die Dicke der Oberlippe verringert und die Exposition der oberen Schneidezähne erhöht. Schließlich würde sich eine Verschlechterung des Malaresdefizits ergeben, die durch die Platzierung von Malaresprothesen kompensiert werden könnte.
2) Wenn ausschließlich eine mandibuläre Retrusion durchgeführt würde, käme es zu einem Verlust der Unterstützung des Weichgewebes der Mandibula mit dem Auftreten eines obtusen cervico-mentalen Winkels und Doppelkinn.
3) Wenn die Chirurgie der mandibulären Retrusion und Mentoplastik kombiniert würde, würde dies ermöglichen, dass der cervico-mentale Winkel nicht verändert wird und kein Doppelkinn auftritt, mit dem zusätzlichen Vorteil der Verbesserung der mentolabialen Furche.
Ziele der präoperativen Kieferorthopädie (Abbildungen 15–25)
1. Die Breite der Bögen beizubehalten, da der beobachtete Kreuzbiss auf die unterschiedliche sagittale Position des Oberkiefers im Vergleich zum Unterkiefer zurückzuführen ist; dieser verschwindet jedoch, wenn die Modelle in Klasse I platziert werden.
2. Die dento-alveolären Kompensationen beseitigen, indem die Schneidezähne korrekt auf ihren knöchernen Basen positioniert werden, das heißt, die Torsion sowohl der oberen als auch der unteren Schneidezähne erhöhen.
3. Die Abweichung der Mittellinie beibehalten, da sie auf eine skelettale Asymmetrie zurückzuführen ist, die in der Chirurgie korrigiert wird.
Im Verlauf der präoperativen Kieferorthopädie wurde eine progressive Sequenz von Bögen verfolgt: 016 Niti thermisch, 018 Niti thermisch, 19x25 Niti thermisch und 19x25 aus Stahl.
Einige Brackets der unteren Schneidezähne wurden erneut zementiert, um eine korrekte Ausrichtung zu erreichen. Nach drei Monaten mit den Stahlbögen wurden vollständige präoperative Aufzeichnungen durch Röntgenaufnahmen, Fotografien und das Montieren von Modellen im Artikulator erstellt. Basierend auf diesen Aufzeichnungen wurde ein finales S.T.O. durchgeführt und die endgültigen chirurgischen Bewegungen der mandibulären Retrusion und der Mentoplastik aus den zuvor genannten Gründen beschlossen.
Einige Tage vor der Operation wurden Stifte in die Bögen eingesetzt, um sie als Unterstützung für die intermaxillären Gummis zu verwenden.







Präoperative Planung
In der präoperativen Planung wurde eine ästhetische Gesichtsdiagnose mit seitlicher cephalometrischer Analyse und Zahnmodellen durchgeführt, die im Artikulator montiert wurden, um die Details der Operation zu planen. Die Modelle wurden eine Woche vor der Operation in einem halbjustierbaren Artikulator in zentrischer Beziehung montiert. Es wurde ein invertierter Überbiss von 7 mm festgestellt.
Es wurde eine mandibuläre Rückverlagerungsoperation geplant, um eine funktionale und ästhetische Okklusion von 9 mm zu erreichen, sowie eine gleitende Osteotomie des Kinns oder Genioplastik mit einer Vorverlagerung von 7 mm und einer vertikalen Verringerung von 2 mm.
Die Entscheidung für die Mentoplastik basiert auf ästhetischen Kriterien, um die Unterstützung der Hauthülle im unteren Drittel des Gesichts nicht zu verlieren, den cervikomandibulären Winkel nicht zu verändern und durch die Verringerung der Höhe und die Vorverlagerung des Kinns den labiomentonischen Winkel zu verbessern.
Chirurgie
Unter Allgemeinanästhesie wurde eine nasotracheale Intubation durchgeführt. Die Inzisionslinien im mandibulären Bereich und am Kinn wurden mit einer Lösung aus Lidocain mit 0,25% und Kochsalzlösung mit Adrenalin 1/100.000 infiltriert; die Osteotomien der Ramus wurden mit der Osteomed-Oszillationssäge durchgeführt, beginnend mit dem horizontalen Schnitt im Ramus und schließlich mit dem vertikalen Schnitt im mandibulären Körper.
Zu jeder Zeit wurde der Schnitt an der äußersten Stelle des Unterkiefers durchgeführt, unmittelbar medial zur äußeren Kortikalis und zur äußeren schrägen Kante. Nach Abschluss der Osteotomie und der Analyse der Integrität des vaskulonervösen Pakets wurde der distale Fragment in der zuvor angefertigten Acrylschiene positioniert und es wurde mit Drähten ein intermaxillärer Zirkelschluss durchgeführt. Ein Knochenfragment wurde vom vorderen Ende des proximalen Fragments oder des Kondylus entfernt, um Interferenzen beim Rückzug des Unterkieferkörpers um 1 cm zu vermeiden. Die Osteotomie wurde mit 3 bikortikalen Schrauben an der äußeren schrägen Kante fixiert; anschließend wurde der passive Sitz des Unterkiefers überprüft, wobei eine angemessene kondyläre Position festgestellt wurde.
Anschließend wurde ein Schnitt im Vestibulum im Bereich der Symphyse durchgeführt, wobei das Kinn und beide Zahnnerven freigelegt wurden; nach Markierung der Mittellinie wurde das Kinn mit einer oszillierenden Säge geschnitten und nach Abschluss der Osteotomie konnte das Kinn frei vorrücken, und dank des Designs der Osteotomie – schräg und nach hinten unten – gingen 3 mm Höhe verloren, was zu einem harmonischeren labiomentonalen Winkel führte.
Die Genioplastik wurde starr mit Osteomed® Platten und vier Schrauben fixiert. Der Verschluss wurde mit 2 Ebenen durchgeführt, um eine Ptosis des Kinns zu vermeiden.
Postchirurgische Kieferorthopädie (Abbildungen 26-36)
Ab der 6. Woche wurde begonnen, eine korrekte Okklusion herzustellen, indem Gummis verwendet wurden, um die Okklusion zu stabilisieren und gegen die Rückfall zu kämpfen.






Diskussion (Abbildungen 37–42)
Die chirurgische Korrektur des Prognathismus bestand traditionell in der posterioren Reposition des mandibulären Körpers mit Ramus-Osteotomien. Dieser Ansatz basiert auf cephalometrischen Studien und hat vorhersehbare und günstige oklusionale sowie funktionale Ergebnisse erzielt. Häufig wurde dieser Ansatz zur Behandlung von Malokklusion und skelettaler Dysharmonie auf Kosten der Gesichtsästhetik gelöst, was zu einem Verlust der Projektion des maxillofazialen Skeletts und einem Verlust der Unterstützung des weichen Gesichtsgewebes führte. Der Verlust von Unterstützung und skelettvolumen führt zu einer Zunahme der Lockerheit, einer Vertiefung der Falten, einer Tendenz zu einem obtuseren cervikomandibulären Winkel und einer Zunahme des Doppelkinns.
Der maxillare Vorstoß stellt eine normale Okklusion her, indem er skelettale Expansion erzeugt und die Hülle erweitert. In diesem Fall wurde jedoch, entgegen der derzeit vorherrschenden Behandlungsmethodik, ausschließlich eine mandibuläre Chirurgie entschieden, basierend auf der folgenden Gesichtsanalys:
- Sehr offener nasolabialer Winkel.
- Unzureichender Nasenrücken für die anthropometrischen Merkmale dieses Falls.
- Gefühl von Prognathismus mit übertriebener anteriorer Divergenz und dem Aussehen eines großen Unterkieferkörpers.
- Makrogenie oder vertikal übermäßig langer Kinn. In diesem Fall hätte jede Art von Oberkiefervorverlagerung zu einer übermäßigen Projektion des Nasenfundaments geführt – was den nasolabialen Winkel noch weiter erhöht hätte – und zur Projektion der Nasenspitze, was ein Aussehen einer Sattelnase zur Folge gehabt hätte, das eine schwierige nachfolgende Nasenchirurgie erforderlich gemacht hätte.
Dem Patienten wurde eine Erhöhung des Jochbeins und des Oberkiefers mit Prothesen angeboten, die er ablehnte. Die mandibuläre Rückverlagerung von 9 mm birgt zwei potenzielle Komplikationen:
- Rückfall.
- Verlust der Unterstützung des Weichgewebes im unteren Drittel des Gesichts und Verschlechterung des cervikomandibulären Winkels.
Der Verlust der Unterstützung der Hauthülle wurde durch eine Vorverlagerung und vertikale Reduktion der Mentoplastik behoben, die das Weichgewebe umverteilte, den labiomentonischen Winkel verbesserte und nicht zu einer Veränderung des cervikomandibulären Winkels mit Zunahme des Doppelkinns führte. Die mandibuläre Rückverlagerung, zusammen mit der Absenkung des Oberkiefers und der transversal Erweiterung des Oberkiefers, sind die instabilsten, unvorhersehbarsten und rückfälligen Bewegungen in der orthognathischen Chirurgie.
Unter allgemeinen Umständen ist der mandibuläre Rückgang vorhersehbar, wenn die skelettale Stabilisierung mit Platten und/oder Schrauben bei allen Osteotomien mit oder ohne Fixierung einer vorgefertigten Schiene sichergestellt ist, die mit Drähten an den Brackets des nicht mobilisierten Oberkiefers verbunden ist, wenn die Magnitude weniger als 7 mm beträgt. In diesen Fällen, wenn es nach der Operation zu einer frühen Malokklusion kommt, ist dies auf einen technischen Fehler während des Eingriffs zurückzuführen.
Bei der späteren Rückfall beeinflussen orthodontische Faktoren wie das Fehlen der Beseitigung zahnärztlicher Kompensationen; oder im Umgang mit transversalen Diskrepanzen oder chirurgischen Faktoren, wie eine unangemessene intraoperative Positionierung des Kondylus, Rotation und Verlust der Kontrolle über den proximalen Ramus, nachdem er distal in der gewünschten Okklusion fixiert wurde, unzureichende Mobilisierung der Fragmente, nach außen gerichtete Rotation des Kondylus aus der Glenoidgrube oder unzureichende Fixierung der Osteotomien; und in vielen Fällen, insbesondere bei Männern, nicht diagnostizierte Kondylhyperplasien oder Patienten, die das Wachstum nicht abgeschlossen haben.
Bei unserem Patienten wurde besonders darauf geachtet, eine passive Fixierung mit den Kondylen an ihrem Platz in der Glenoidhöhle zu erreichen, ohne Verdrehungen, und dass beim Entfernen von 1 cm Knochenfragmenten keine Interferenzen in der Position beider Osteotomien bestehen. Die zentrische Beziehung wurde im Operationssaal mehrfach überprüft und es wurden weiche Gummibänder der Klasse
III platziert. Unsere Erfahrung mit Klasse III und bikortikalen Schrauben ist äußerst zufriedenstellend und bietet einen hohen Stabilitätsgrad mit minimalem Schraubeneinsatz im Unterkiefer.



César Colmenero Ruiz, Fe Serrano Madrigal, Javier Prieto Serrano
Bibliografie
- Rosen HM. Maxilläre Vorverlagerung bei mandibulärem Prognathismus: Indikationen und Begründung. Plast Reconstr Surg 87: 823-831, 1991.
- Epker B, Fisch I. Die chirurgisch-orthodontische Korrektur des Klasse III skeletalen offenen Bisses. Am J Orthod Dentofacial Orthop 73: 601-617, 1978.
- Kobayashi T, Hoshima T. Kaumuskelfunktion bei Patienten mit mandibulärem Prognathismus vor und nach der orthognathischen Chirurgie. J Oral Maxillofac Surg 51: 997-1004, 1993.
- Proffit Wr, Philips C, Dann C. Stabilität nach chirurgisch-orthodontischer Korrektur des skeletalen Klasse III. Int. J Adult Orthod Orthognath Surg 6: 7-14, 1991.
- Obwegeser HL. Anomalien des mandibulären Wachstums. Springer-Verlag: 332-335, 2000.
- Spiessl B. Die sagittale Spaltosteotomie zur Korrektur des mandibulären Prognathismus. Scand J Plast Reconstr Surg Hand Surg 9: 496-502, 1982.
- Rosen HM. Ästhetische Richtlinien und Verfeinerungen in der Genioplastik: die Rolle des labiomentalen Goldes. Plast Reconstr Surg 88: 5, 14, 1991.
- Wolfe SA. Verkürzung und Verlängerung des Kinns. J Craneomaxillofac Surg 15: 223-228, 1987